Cleft malformations and malformation surgery
The most common congenital malformations in the head and neck region and malocclusions caused by them are treated and cared for by our experienced team. We have highly developed therapies and surgical techniques that ensure that hardly any scars are visible afterwards and that the face and dentition continue to develop in a healthy and harmonious way.
Patient videos – jaw
Patient videos – face
Malformation surgery
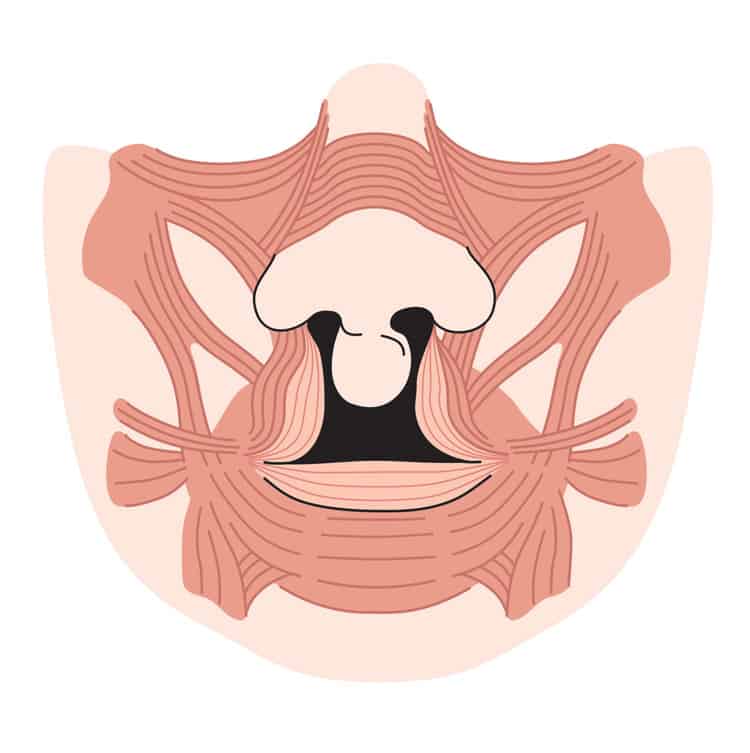
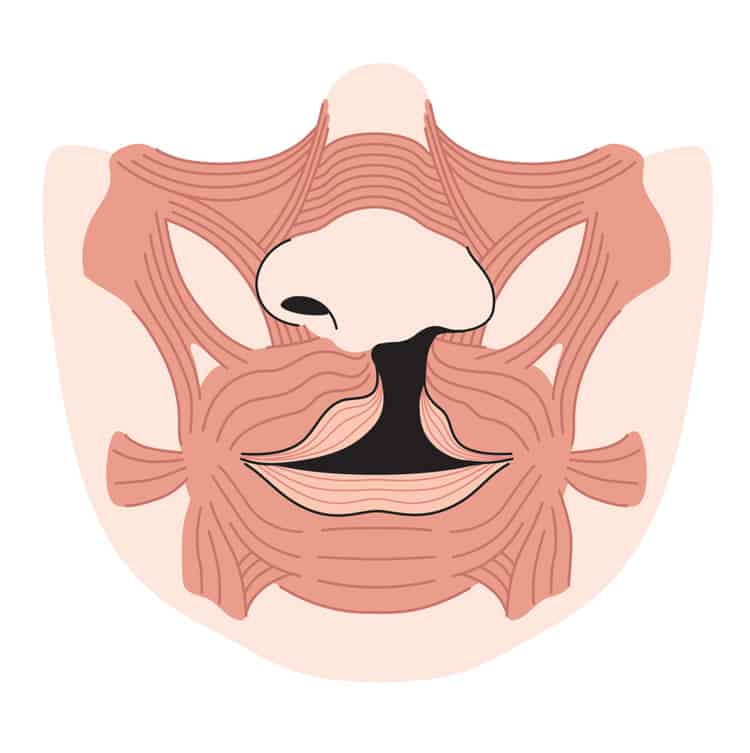
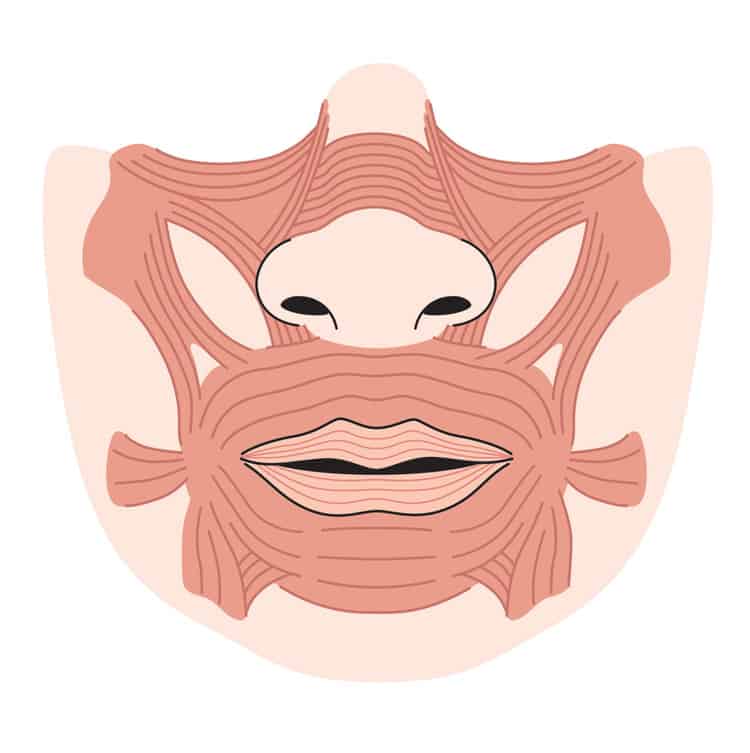
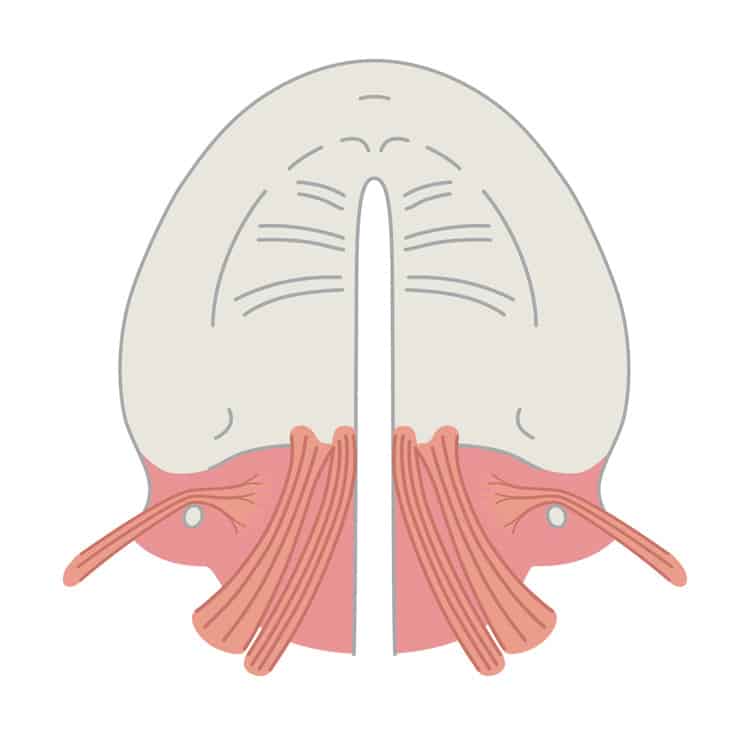
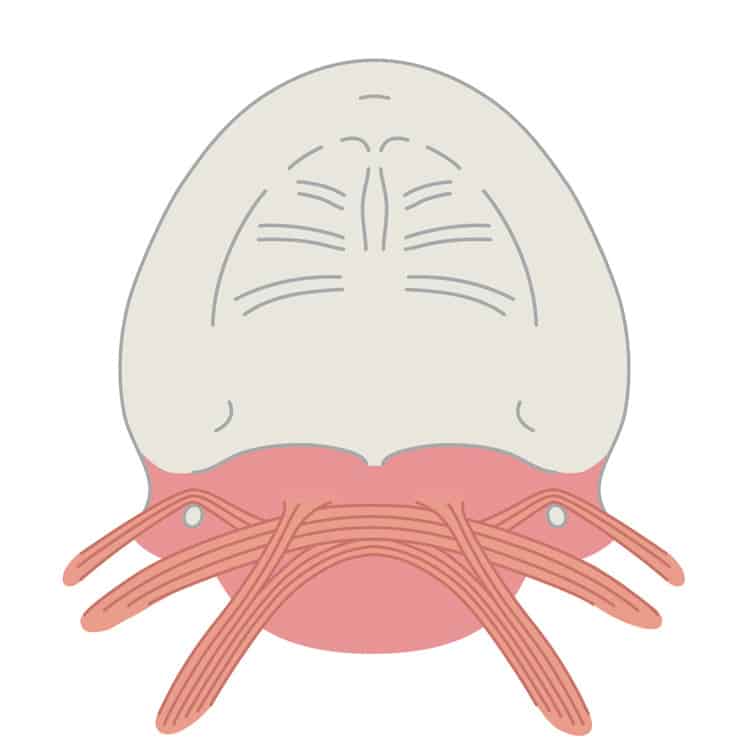
The most common congenital malformation in the head and neck region is the cleft lip, jaw and palate. Cleft lips, jaws and palates are the most common neonatal malformation, with one newborn with a cleft per 500 births. We can correct them so that almost no visible scars remain.
In the vast majority of cases, a cleft is detected during the ultrasound examination in pregnancy. We will be happy to advise you on this even before the birth of your child. Please simply make an appointment by calling +49 (0)69 8405-1380 or sending an e-mail









Example of a course of treatment for the Pierre Robin sequence







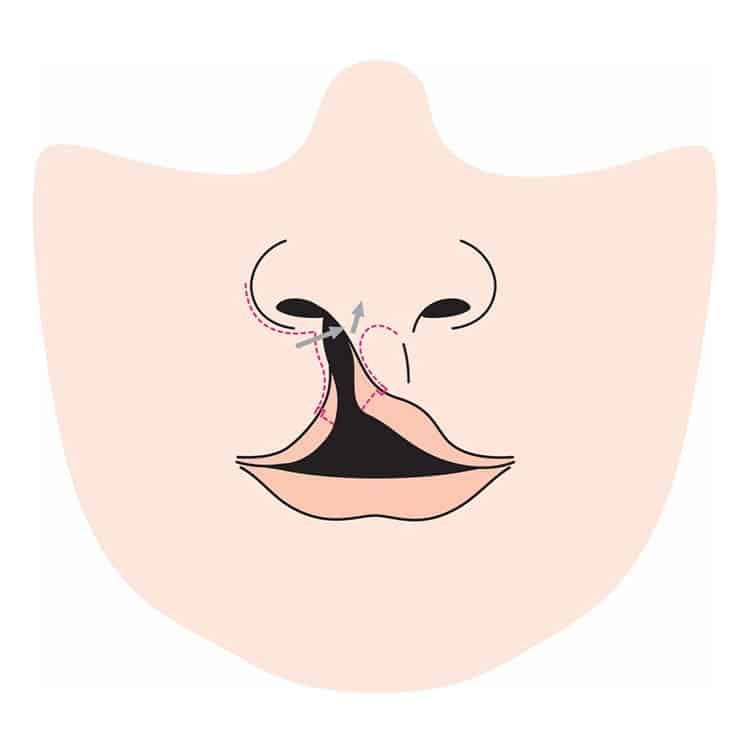
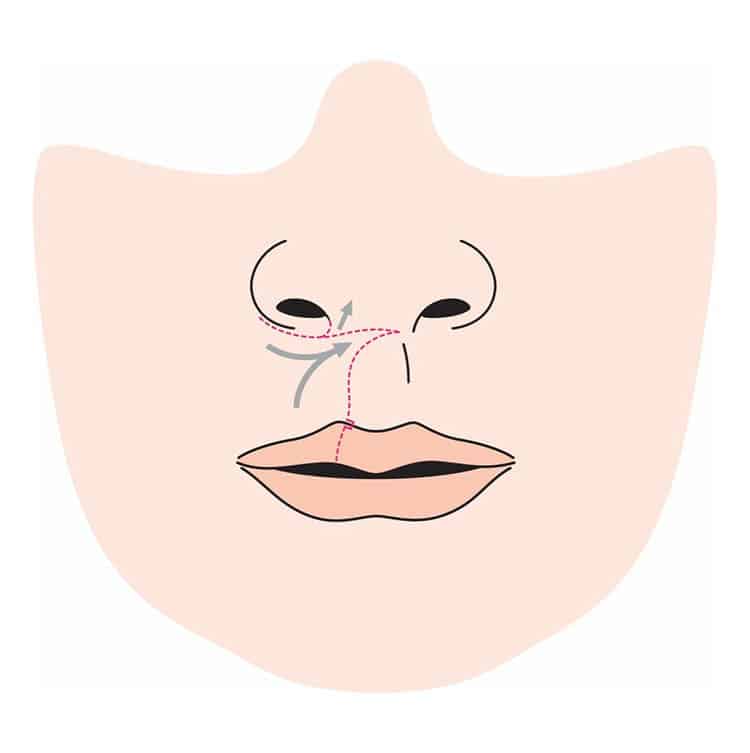
Cleft rhinoplasties


























Jaw realignments in cleft patients
These patients first had a jaw realignment followed by a lip and nose operation (lip rhinoplasty). Figure A shows the before and after comparison of the jaw realignment, Figure 1C, 1D, 2B and 2C show the patients before and after the lip rhinoplasty.

We treat bones with gentle ultrasound (demonstrated here on a raw egg)
Are you looking for help?
We will be happy to advise you on the possibilities of conservative or surgical treatment of your health problem affecting the mouth, jaw or facial area. We’re happy to help! You can reach the Landes & Kollegen Practice by telephone on +49 (0) 69 8405-1380 or by e-mail.
All planned surgical treatments are preceded by a detailed consultation, which can also take place several times and repeatedly.
We speak German, English, French, Spanish, Arabic and Portuguese.
Our regular office hours are:
Monday, Tuesday, Thursday: 8:00 – 17:00, Wednesday: 8:00 – 13:00, Friday: 8:00 – 16:00
as well as our fast-track consultations on Tuesday, Thursday and Friday, between 8:00 and 9:00 each day!
The new me as a 3D simulation
Design your own dream face! Simply upload selfies, simulate them free of charge with the Crisalix 3D software and bring them to your appointment with us!